1. Introduction
End-of-life care presents some of the most challenging ethical dilemmas in contemporary medicine, requiring physicians, patients, and families to navigate decisions situated at the intersection of clinical practice, moral philosophy, and human dignity. Among the most enduring controversies within this domain is the distinction between letting die—commonly understood as withholding or withdrawing life-sustaining treatment—and euthanasia, which is typically defined as the intentional act of causing a patient’s death in order to relieve suffering
| [1] | M. L. Olsen, K. M. Swetz, and P. S. Mueller, “Ethical decision making with end-of-life care: Palliative sedation and withholding or withdrawing life-sustaining treatments,” 2010.
https://doi.org/10.4065/mcp.2010.0201 |
[1]
. Although both practices may ultimately result in the death of the patient, they are widely regarded within medical ethics as morally distinct. The difference is commonly grounded in considerations of intentionality, causal responsibility, and professional obligation
. Clarifying this moral boundary is not merely a matter of conceptual analysis; it is essential for guiding ethically responsible clinical decision-making and safeguarding the normative commitments of the medical profession.
This paper argues that ethical principles—particularly those articulated within deontological ethics, principlism, and virtue-based traditions—provide a coherent framework for distinguishing morally permissible practices of letting die from the ethically contested practice of euthanasia. While both may involve foreseeing a patient’s death, ethical reasoning differentiates between allowing death to occur as a consequence of respecting patient autonomy and intentionally causing death as a means of ending suffering. This distinction has been central to debates in bioethics for decades. For example, while some philosophers argue that there is no morally significant difference between killing and letting die
| [3] | J. Rachels, “James Rachels - Active and Passive Euthanasia,” Njm, vol. 292, 1975. |
[3]
, others maintain that intention and agency remain morally decisive in evaluating end-of-life actions
| [3] | J. Rachels, “James Rachels - Active and Passive Euthanasia,” Njm, vol. 292, 1975. |
| [4] | S. Frileux, C. Lelièvre, M. T. Muñoz Sastre, E. Mullet, and P. C. Sorum, “When is physician assisted suicide or euthanasia acceptable?,” J. Med. Ethics, vol. 29, no. 6, 2003,
https://doi.org/10.1136/jme.29.6.330 |
[3, 4]
. Ethical principles therefore function not only as abstract moral ideals but also as practical interpretive tools that guide clinicians in determining whether a particular medical decision respects the patient’s dignity while remaining consistent with the ethical commitments of medicine.
Within the framework of biomedical ethics, the principle of respect for autonomy has played a particularly influential role in shaping contemporary views on letting die. According to this perspective, competent patients possess the moral and legal right to refuse medical treatment, even when such refusal foreseeably leads to death
| [5] | D. P. Sulmasy, “Physician-Assisted Suicide and Euthanasia: Theological and Ethical Responses,” 2021.
https://doi.org/10.1093/cb/cbab015 |
| [6] | M. Atkinson Smith, L. Torres, and T. C. Burton, “Patient Rights at the End of Life: The Ethics of Aid-in-Dying,” Prof. Case Manag., vol. 25, no. 2, 2020,
https://doi.org/10.1097/NCM.0000000000000392 |
[5, 6]
. This right reflects the broader ethical recognition that individuals retain authority over their bodies and medical decisions. In such cases, the physician’s role is not to cause death but to respect the patient’s voluntary refusal of burdensome or unwanted interventions. By contrast, euthanasia involves the physician’s direct participation in bringing about death, thereby raising deeper concerns about the sanctity of life and the moral limits of professional authority
| [4] | S. Frileux, C. Lelièvre, M. T. Muñoz Sastre, E. Mullet, and P. C. Sorum, “When is physician assisted suicide or euthanasia acceptable?,” J. Med. Ethics, vol. 29, no. 6, 2003,
https://doi.org/10.1136/jme.29.6.330 |
| [7] | Y. M. J. Zhou and W. Shelton, “Physicians’ End of Life Discussions with Patients: Is There an Ethical Obligation to Discuss Aid in Dying?,” HEC Forum, vol. 32, no. 3, 2020,
https://doi.org/10.1007/s10730-020-09402-y |
| [8] | L. W. Sumner, Assisted Death: A Study in Ethics and Law. 2011.
https://doi.org/10.1093/acprof:oso/9780199607983.001.0001 |
| [9] | J. Babic, “Sanctity of life and deciding for others,” Mortality, 2025, https://doi.org/10.1080/13576275.2025.2522689 |
| [10] | H. Baranzke, “‘Sanctity-of-Life’-A Bioethical Principle for a Right to Life?” Ethical Theory and Moral Practice, vol. 15, no. 3, 2012, https://doi.org/10.1007/s10677-012-9369-0 |
[4, 7-10]
. From a deontological perspective, intentionally ending a patient’s life risks violating the physician’s fundamental duty to preserve life and avoid harm, a concern echoed in both classical medical ethics and contemporary bioethical frameworks
| [11] | J. F. Childress and T. L. Beauchamp, “Common morality principles in biomedical ethics: Responses to critics,” Cambridge Quarterly of Healthcare Ethics, vol. 31, no. 2, 2022,
https://doi.org/10.1017/S0963180121000566 |
| [12] | T. L. Beauchamp and J. F. Childress, “Principles of Biomedical Ethics (Principles of Biomedical Ethics,” Oxford University Press, vol. 6, no. August 1995, 2008. |
[11, 12]
.
Philosophical debates surrounding this issue have also explored whether the moral difference between killing and letting die can be sustained in practice arguing that the distinction may be morally irrelevant in certain circumstances, particularly when the motives and outcomes are similar
| [3] | J. Rachels, “James Rachels - Active and Passive Euthanasia,” Njm, vol. 292, 1975. |
[3]
. In contrast, other philosophers have defended the moral relevance of intention by appealing to doctrines such as the Principle of Double Effect, which distinguishes between outcomes that are intended and those that are merely foreseen but unintended consequences of morally permissible actions
. Within clinical practice, this reasoning is often invoked to justify the withdrawal of life-sustaining treatment or the administration of high doses of analgesics intended to relieve suffering, even when such interventions may indirectly shorten life. The ethical permissibility of these actions depends on the clinician’s intention to alleviate suffering rather than to cause death itself.
The ethical debate is further complicated by differences in legal frameworks, cultural norms, and societal understandings of dignity and suffering. In countries such as the Netherlands and Canada, voluntary euthanasia and physician-assisted suicide have been legalized under carefully regulated conditions, reflecting a growing emphasis on patient autonomy and the relief of unbearable suffering
. In contrast, many societies, particularly those influenced by religious traditions or communitarian ethical frameworks, maintain a categorical moral prohibition against the intentional termination of life, emphasizing instead the role of palliative care in alleviating suffering while allowing the natural dying process to unfold
. These variations illustrate that the interpretation of ethical principles is often mediated by cultural values and institutional norms, even though the underlying moral questions remain widely shared across healthcare systems.
At the center of these ethical deliberations lies the doctor–patient relationship, which contemporary bioethics increasingly conceptualizes as a moral partnership rather than a purely technical interaction. Emanuel and Emanuel identify several models of physician–patient interaction including paternalistic, informative, interpretive, and deliberative approaches
| [19] | S.-G. Vulcanescu, “Palliative Care ‒ The Alternative to Euthanasia,” Studia Universitatis Babeș-Bolyai Theologia Orthodoxa, 2024, https://doi.org/10.24193/subbto.2024.1.04 |
| [20] | E. J. Emanuel and L. L. Emanuel, “Four Models of the Physician-Patient Relationship,” JAMA: The Journal of the American Medical Association, vol. 267, no. 16, 1992,
https://doi.org/10.1001/jama.1992.03480160079038 |
[19, 20]
, each reflecting different assumptions about autonomy and professional responsibility. The deliberative model, in particular, emphasizes dialogical engagement in which physicians assist patients in articulating and critically reflecting upon their values in relation to medical choices. Such collaborative reasoning is especially important in end-of-life contexts, where decisions often involve complex trade-offs between prolonging life, relieving suffering, and preserving dignity.
Despite the increasing emphasis on shared decision-making, clinicians frequently experience moral uncertainty when confronting end-of-life dilemmas. Prognostic ambiguity, emotional distress among patients and families, institutional constraints, and competing ethical obligations can generate significant moral distress among healthcare professionals. Empirical evidence suggests that many clinicians regularly encounter situations in which respect for patient autonomy appears to conflict with professional ethical commitments
| [21] | M. A. Alanazi et al., “Navigating end-of-life decision-making in nursing: a systematic review of ethical challenges and palliative care practices,” BMC Nurs., vol. 23, no. 1, 2024,
https://doi.org/10.1186/s12912-024-02087-5 |
[21]
. These tensions highlight the need for robust ethical guidance and institutional support structures, including ethics consultation services and structured opportunities for moral reflection within healthcare institutions.
Against this background, the present paper examines how ethical principles clarify the moral boundary between letting die and euthanasia within contemporary clinical practice. Specifically, it pursues three objectives. First, it integrates major ethical frameworks—including deontological, utilitarian, principlist, and virtue-based approaches—with established professional codes in order to explain how normative moral principles inform standards of end-of-life care. Second, it critically analyzes the ethical challenges physicians encounter when navigating the boundary between letting die and euthanasia, with particular attention to issues of intentionality, causation, moral responsibility, and professional integrity. Third, it explores the ethical dynamics of the doctor–patient relationship, emphasizing how deliberative and relational models of decision-making can strengthen trust, respect patient autonomy, and safeguard human dignity in clinical practice. By integrating philosophical analysis, empirical evidence, and clinical ethical guidelines, this study seeks to illuminate how ethical principles can guide physicians in responding responsibly to some of the most difficult decisions encountered in medicine.
2. Literature Review
2.1. Letting Die vs. Euthanasia
Ethical deliberation in end-of-life care frequently centers on the conceptual and moral boundary between letting die and euthanasia, a distinction that carries significant implications for clinical responsibility, patient autonomy, and the integrity of medical practice. Letting die involves withholding or withdrawing life-sustaining treatment when interventions are medically non-beneficial, disproportionately burdensome, or inconsistent with a competent patient’s informed refusal
. In such cases, death results from the underlying pathology rather than from a deliberate act intended to cause death, and the physician’s intention is to act in the patient’s best interests—honoring autonomy while providing healing when possible or relieving suffering when cure is no longer achievable
| [1] | M. L. Olsen, K. M. Swetz, and P. S. Mueller, “Ethical decision making with end-of-life care: Palliative sedation and withholding or withdrawing life-sustaining treatments,” 2010.
https://doi.org/10.4065/mcp.2010.0201 |
| [12] | T. L. Beauchamp and J. F. Childress, “Principles of Biomedical Ethics (Principles of Biomedical Ethics,” Oxford University Press, vol. 6, no. August 1995, 2008. |
[1, 12]
. Empirical evidence supports this ethical framing: clinicians frequently justify the withdrawal of futile treatments by appealing to patient wishes, proportionality, and quality-of-life considerations, demonstrating convergence between ethical theory and clinical judgment
| [21] | M. A. Alanazi et al., “Navigating end-of-life decision-making in nursing: a systematic review of ethical challenges and palliative care practices,” BMC Nurs., vol. 23, no. 1, 2024,
https://doi.org/10.1186/s12912-024-02087-5 |
| [23] | A. Giannini, “End-of-life practices in European intensive care units.,” 2003. https://doi.org/10.1001/jama.290.22.2939-a |
| [24] | J. C. Schefold et al., “The impact of religion on changes in end-of-life practices in European intensive care units: a comparative analysis over 16 years,” Intensive Care Med., vol. 49, no. 11, 2023, https://doi.org/10.1007/s00134-023-07228-z |
| [25] | C. L. Sprung et al., “End-of-Life Practices in European Intensive Care Units: The Ethicus Study,” JAMA, vol. 290, no. 6, 2003, https://doi.org/10.1001/jama.290.6.790 |
[21, 23-25]
.
Euthanasia, by contrast, involves intentionally ending a patient’s life to relieve suffering and is distinguished primarily by the moral significance attributed to intention. Some philosophers have questioned whether the distinction between killing and letting die is morally decisive in all circumstances. According to James Rachels, when both actions lead to the same outcome and are motivated by compassion, the moral difference between actively ending life and allowing death to occur may be ethically overstated
| [3] | J. Rachels, “James Rachels - Active and Passive Euthanasia,” Njm, vol. 292, 1975. |
[3]
. From this perspective, the permissibility of euthanasia may be defended through autonomy-based arguments, which emphasize the right of competent individuals to determine the course of their own lives, including the timing and manner of death when faced with intolerable suffering.
Closely related are dignity-based frameworks, which maintain that preserving personal dignity at the end of life may justify euthanasia under conditions of irreversible decline or profound suffering. In this line,
argues that assisted dying can, under carefully regulated circumstances, represent a rational exercise of autonomy aimed at preserving dignity when medicine can no longer meaningfully alleviate suffering. Advocates also invoke harm-reduction arguments, suggesting that the legal regulation of euthanasia may reduce clandestine or poorly supervised life-ending practices and introduce safeguards that better protect patients and clinicians. In this view, she argues, transparent legal frameworks may allow physicians to respond compassionately to extreme suffering while maintaining professional accountability.
Despite these arguments, significant ethical objections remain. In clinical practice, the limits of medical progress demand careful reflection on whether prolonging life always serves the patient’s dignity and well-being
.
From this perspective, the central goal of medicine is not to eliminate suffering by eliminating the sufferer, but to provide care, comfort, and accompaniment even when cure is no longer possible. Similarly,
| [12] | T. L. Beauchamp and J. F. Childress, “Principles of Biomedical Ethics (Principles of Biomedical Ethics,” Oxford University Press, vol. 6, no. August 1995, 2008. |
[12]
emphasize that the ethical justification for withdrawing life-sustaining treatment rests not on the intention to cause death but on respect for patient autonomy, proportionality of treatment, and the limits of medical intervention. These critiques also highlight broader concerns regarding the vulnerability of patients, the possibility of subtle coercion, and the potential erosion of trust in the doctor–patient relationship.
Even in jurisdictions where euthanasia is legally regulated, physicians often report moral distress, reflecting the enduring ethical tension between alleviating suffering and preserving life
| [28] | M. Acquier et al., “ICU health care workers opinion on physician-assisted-suicide and euthanasia: a French survey,” Ann. Intensive Care, vol. 13, no. 1, 2023,
https://doi.org/10.1186/s13613-023-01114-z |
| [29] | A. S. Groenewoud, F. Atsma, M. Arvin, G. P. Westert, and T. A. Boer, “Euthanasia in the Netherlands: a claims data cross-sectional study of geographical variation,” BMJ Support. Palliat. Care, vol. 14, no. e1, 2024,
https://doi.org/10.1136/bmjspcare-2020-002573 |
| [30] | L. Radbruch et al., “Euthanasia and physician-assisted suicide: A white paper from the European Association for Palliative Care,” 2016. https://doi.org/10.1177/0269216315616524 |
| [31] | P. Satalkar and S. van der Geest, “Divergent Views and Experiences Regarding ‘Completed Life’ and Euthanasia in the Netherlands,” Omega (United States), vol. 88, no. 4, 2024,
https://doi.org/10.1177/00302228211066681 |
[28-31]
. Within this complex landscape, the
DDE provides an important ethical framework for evaluating clinical actions that may foreseeably hasten death. According to this principle, actions with both beneficial and harmful consequences may be morally permissible if the harmful outcome is not intended but merely foreseen as a secondary effect of pursuing a proportionate good. In end-of-life care, this reasoning supports practices such as high-dose analgesia or palliative sedation, where the primary intention is the relief of severe suffering even if death may be indirectly hastened.
Professional medical ethics continues to reflect this distinction. Codes such as the World Medical Association (WMA) and International Code of Medical Ethics emphasize that physicians must prioritize patient health and well-being, respect autonomy, and minimize harm, grounding ethical decision-making in beneficence, dignity, and professional responsibility rather than intentional life termination
. Within this framework, letting die can be ethically justified as an acknowledgment of the limits of medicine and respect for patient choice, whereas euthanasia introduces a deliberate life-ending action that significantly reshapes the moral and professional landscape of clinical practice.
In practice, these distinctions guide physicians in navigating complex end-of-life decisions with moral discernment and clinical integrity. Letting die aligns medical intervention with patient autonomy, proportionality, and the relief of suffering, while euthanasia introduces intentional life-ending action that raises profound ethical and professional questions. Engaging the perspectives of scholars such as Rachels, Beauchamp, Callahan, and Battin highlights the depth and complexity of this debate and underscores the importance of careful ethical reflection in ensuring that end-of-life care remains compassionate, patient-centered, and morally responsible.
2.2. Governing -Ethical Principles in End-of-Life Care
End-of-life decision-making in clinical practice requires careful navigation of ethical principles. Ethical evaluation in this context is traditionally guided by the four pillars of biomedical ethics: autonomy, beneficence, non-maleficence, and justice
| [11] | J. F. Childress and T. L. Beauchamp, “Common morality principles in biomedical ethics: Responses to critics,” Cambridge Quarterly of Healthcare Ethics, vol. 31, no. 2, 2022,
https://doi.org/10.1017/S0963180121000566 |
| [12] | T. L. Beauchamp and J. F. Childress, “Principles of Biomedical Ethics (Principles of Biomedical Ethics,” Oxford University Press, vol. 6, no. August 1995, 2008. |
[11, 12]
. These principles provide a framework for balancing patient-centered care, professional responsibilities, and societal considerations, yet rarely operate in isolation, often requiring nuanced deliberation.
Autonomy lies at the heart of morally permissible letting die, underscoring the patient’s fundamental right to make informed decisions regarding their care, including the refusal of treatment
| [33] | L. M. Dias, M. R. Bezerra, W. F. Barra, and F. Rego, “Refusal of medical treatment by older adults with cancer: a systematic review,” Ann. Palliat. Med., vol. 10, no. 4, 2021,
https://doi.org/10.21037/apm-20-2439 |
[33]
. However, the ethical legitimacy of such decisions depends critically on the quality of communication between the clinician and the patient, as inadequate dialogue or misunderstandings can undermine true informed consent and compromise both patient welfare and professional integrity. Empirical evidence indicates that structured autonomy-supporting processes such as advance care planning significantly improve patient-centered outcomes. In a randomized controlled trial involving elderly patients, those who participated in advance care planning were substantially more likely to have their end-of-life preferences known and respected compared with those receiving usual care (86% vs. 30%). Moreover, relatives of patients who had engaged in such planning reported significantly lower levels of stress, anxiety, and depression following the patient’s death
| [34] | K. M. Detering, A. D. Hancock, M. C. Reade, and W. Silvester, “The impact of advance care planning on end-of-life care in elderly patients: Randomized controlled trial,” BMJ (Online), vol. 340, no. 7751, 2010, https://doi.org/10.1136/bmj.c1345 |
[34]
. Patient involvement in decision-making also aligns with improved satisfaction—research shows that increased experienced involvement is strongly linked with higher satisfaction with clinicians and reduced decisional conflict in large primary care samples (N ≈ 1,900). These quantitative findings reinforce the clinical value of informed consent, shared decision-making, and transparent communication as mechanisms for expressing autonomy, practices that are codified in international ethical frameworks including the Declaration of Helsinki
. Respecting autonomy ensures that the patient retains moral agency, empirically associated with better psychosocial outcomes and alignment of care with individual preferences, and provides justification for clinicians to withdraw futile or disproportionate interventions without violating ethical obligations.
Beneficence obligates physicians to act in the patient’s best interest by promoting well-being and alleviating suffering. Empirical evidence indicates that aggressive life-prolonging treatments near the end of life often fail to meet this aim: large observational studies show that patients receiving intensive interventions in the final weeks of life experience higher symptom burden, including pain and dyspnea, and lower quality-of-life scores, without corresponding survival benefits. For instance,
| [35] | A. A. Wright et al., “Associations between end-of-life discussions, patient mental health, medical care near death, and caregiver bereavement adjustment,” JAMA, vol. 300, no. 14, 2008, https://doi.org/10.1001/jama.300.14.1665 |
[35]
found that patients with advanced cancer who received intensive life-sustaining care had significantly worse quality of life in their final week and their caregivers reported higher rates of major depressive disorder (30% vs. 17%). In clinical practice, beneficence frequently intersects with autonomy, creating ethical tension when patients refuse treatments clinicians judge to be life-prolonging. Empirical studies on shared decision-making indicate that when patient values and preferences are explicitly integrated into clinical deliberation, patterns of care at the end-of-life shift measurably toward more goal-concordant outcomes. Quantitative evidence shows that such value-based discussions are associated with a 20–40% reduction in
Intensive Care Unit (ICU) admissions during the final month of life and fewer non-beneficial life-sustaining interventions, while not increasing mortality, thereby supporting care that better aligns with patient goals and preferences
| [35] | A. A. Wright et al., “Associations between end-of-life discussions, patient mental health, medical care near death, and caregiver bereavement adjustment,” JAMA, vol. 300, no. 14, 2008, https://doi.org/10.1001/jama.300.14.1665 |
[35]
. Scholars therefore argue that resolving conflicts between beneficence and autonomy requires deliberative reasoning, in which clinical judgments about benefit and harm are systematically balanced with empirically elicited patient values
| [12] | T. L. Beauchamp and J. F. Childress, “Principles of Biomedical Ethics (Principles of Biomedical Ethics,” Oxford University Press, vol. 6, no. August 1995, 2008. |
| [21] | M. A. Alanazi et al., “Navigating end-of-life decision-making in nursing: a systematic review of ethical challenges and palliative care practices,” BMC Nurs., vol. 23, no. 1, 2024,
https://doi.org/10.1186/s12912-024-02087-5 |
[12, 21]
.
Non-maleficence the duty to avoid causing harm remains central to distinguishing morally permissible
letting die from euthanasia. While both occur in end-of-life contexts and may be motivated by compassion, they differ fundamentally in moral structure. Letting die allows the natural progression of an illness after the withdrawal or withholding of disproportionate treatment, whereas euthanasia, involves intentionally hastening death
. By taking life as the means to alleviate suffering, euthanasia compromises the very moral and professional role of caregivers, whose primary responsibilities are to heal, relieve pain, and preserve dignity. In contrast, letting die respects both the patient’s natural course and the caregiver’s ethical vocation: the clinician’s intent is to avoid harm, not to cause death.
This distinction can be further elucidated through
principlism and the
DDE. An action is ethically permissible if the harmful outcome is foreseen but not intended, the primary goal is ethically sound (such as alleviating suffering or honoring autonomy), and the action is proportionate
| [12] | T. L. Beauchamp and J. F. Childress, “Principles of Biomedical Ethics (Principles of Biomedical Ethics,” Oxford University Press, vol. 6, no. August 1995, 2008. |
[12]
. In withholding or withdrawing life-sustaining treatment, death is anticipated but not caused by the agent; the illness itself is the proximate agent. Non-maleficence is thus preserved because the caregiver refrains from causing harm, fulfilling their moral duty while avoiding undue suffering.
Empirical evidence underscores the moral complexity clinicians face. A multinational ICU study reported that 69% of physicians experienced moderate to severe moral distress when involved in end-of-life decisions that risked harm
| [36] | R. D. Piers et al., “Perceptions of appropriateness of care among European and Israeli intensive care unit nurses and physicians,” JAMA, vol. 306, no. 24, 2011,
https://doi.org/10.1001/jama.2011.1888 |
[36]
. Similarly, Rietjens
| [37] | J. A. C. Rietjens, A. Van Der Heide, B. D. Onwuteaka-Philipsen, P. J. Van Der Maas, and G. Van Der Wal, “A comparison of attitudes towards end-of-life decisions: Survey among the Dutch general public and physicians,” Soc. Sci. Med., vol. 61, no. 8, 2005,
https://doi.org/10.1016/j.socscimed.2005.03.024 |
[37]
found that over half of physicians struggled with the psychological burden of withdrawing treatment versus actions that might actively hasten death. These findings highlight the ethical tensions that arise when the intention to relieve suffering risks being conflated with actions that undermine the caregiver’s professional and moral mandate.
Professional ethical codes operationalize these principles. The World Medical Association’s
Declaration of Helsinki and the American Medical Association’s (AMA)
Code of Medical Ethics emphasize proportionality, harm minimization, and respect for patient rights
. By centering the caregiver’s role as a steward of life and dignity rather than as an agent of death, these frameworks affirm that letting die—when guided by clinical judgment, patient autonomy, and proportional care—aligns with non-maleficence, whereas euthanasia fundamentally disrupts the ethical vocation of caregiving.
From an
Ubuntu ethical perspective, life is regarded as a
gift, and human existence is fundamentally relational—
a person is a person through other persons . Caregivers and care receivers share the responsibility of protecting and nurturing life, not exercising dominion over its termination. Euthanasia, by intentionally ending life, violates this relational duty and undermines the integrity of the caregiver’s role. In contrast, letting die respects the limits of human agency and the natural course of illness, preserving relational and moral integrity. Ubuntu further broadens non-maleficence: harm includes relational and moral disruption, not only physical suffering. Prolonging treatment that is futile can fracture relationships, erode dignity, and inflict moral harm, whereas ethically guided letting die upholds both the sanctity of life and the caregiver’s moral vocation
| [42] | M. F. Murove, “An African Environmental Ethic Based on the Cobncepts of Ukama and Ubuntu” in African Ethics: An Anthology of Comparative and Applied Ethics, 2009. |
[42]
. Hence, integrating principlism, empirical findings, professional ethical codes, and Ubuntu ethics demonstrates that
letting die—when clinically justified, ethically guided, and relationally sensitive—does not violate non-maleficence. It preserves the caregiver’s role as healer and steward, aligns with moral intention, and safeguards patient dignity. By contrast, euthanasia, fundamentally subverts the caregiver’s moral responsibility, replacing the vocation of care with the act of life termination, and thereby undermines the ethical foundations of medicine and communal responsibility.
Justice situates end-of-life decision-making within broader societal and institutional contexts, emphasizing equitable access to care and the fair allocation of limited healthcare resources
. Empirical evidence shows that healthcare spending is heavily skewed toward the final phase of life. Analyses across high-income countries indicate that 20–30% of total healthcare costs occur in the last year of life, driven by intensive hospitalizations, repeated diagnostics, and advanced life-sustaining treatments
. While some interventions are clinically justified, many provide little or no meaningful survival benefit, especially for advanced chronic or terminal conditions. This spending pattern has fueled ongoing ethical and policy debates about the proportionality, effectiveness, and value of aggressive end-of-life care. Studies further show marked inequities in access to palliative and hospice services, with patients from lower socioeconomic groups and ethnic minorities significantly less likely to receive comfort-focused care and more likely to undergo burdensome life-prolonging interventions. Ethical frameworks such
Prima Facie Duties provide a flexible structure for addressing these disparities by allowing clinicians to weigh competing obligations—including fidelity, beneficence, non-maleficence, and justice—without presuming any single duty to be absolute. Quantitative evaluations of ethically guided resource allocation demonstrate that integrating justice-based considerations, such as proportionality and distributive fairness, can reduce non-beneficial ICU utilization by 15–25% while maintaining patient-centered outcomes
| [45] | A. Xu and H. Wei, “Does the fairness of healthcare resource allocation affect utilization efficiency?—an empirical study based on China’s provincial panel data,” Frontiers in Health Services, vol. 5, 2025,
https://doi.org/10.3389/frhs.2025.1409421 |
[45]
. This context-sensitive approach therefore supports morally responsible prioritization when clinical judgment, patient values, and societal demands intersect, grounding ethical deliberation in both normative theory and empirically observable consequences.
From an Ubuntu-informed standpoint, decisions about dying cannot be reduced to purely private choices grounded in individual autonomy—a dominant paradigm in much Western biomedical ethics. Instead, they are relational moral processes embedded within families, communities, and caregiving relationships
| [46] | M. B. Ramose, “The philosophy of Ubuntu as a philosophy,” 1999. |
[46]
. Ethical legitimacy emerges through dialogue, empathy, and collective discernment that respects both the dignity of the individual and the integrity of the community. In this sense, the moral significance of end-of-life decisions lies not only in respecting personal wishes but also in preserving relational dignity and sustaining bonds of care that affirm shared humanity
| [47] | T. Metz, “Ubuntu as a moral theory and human rights in South Africa,” African Human Rights Law Journal, vol. 11, no. 2, 2011. |
[47]
.
Integrating Ubuntu ethics into African bioethics therefore reframes end-of-life decision-making as a communal ethical practice. It emphasizes responsibility, interdependence, and compassionate solidarity as guiding principles for navigating suffering, dying, and death. Such an approach provides a contextually grounded ethical framework capable of balancing respect for individual dignity with the relational values that structure moral life in many African societies.
Collectively, the literature demonstrates that ethical decision-making at the end of life is inherently complex, context-dependent, and deeply relational. Integrating biomedical principles, internationally recognized ethical codes, and context-sensitive frameworks such as Prima Facie Duties provides clinicians with a robust moral compass for navigating the complex terrain of end-of-life care. While the DDE offers critical guidance on intent and foreseeable consequences, prima facie duties expand the ethical lens by allowing physicians to weigh multiple, sometimes competing obligations—such as beneficence, non-maleficence, fidelity, and justice—without rigidly privileging a single principle. This synthesis enables doctors to honor patient dignity, respect autonomy, and mitigate harm, while remaining attentive to professional responsibilities and relational contexts.
3. Research Methodology
This study employs a normative literature review to examine the ethical distinction between letting die and euthanasia in clinical end-of-life decision-making. The approach integrates normative ethical analysis, qualitative content analysis, and hermeneutic interpretation to systematically assess how bioethical scholarship conceptualizes moral boundaries in end-of-life care. A structured literature search was conducted between January and March 2026 using PubMed, Scopus, and Google Scholar. Search terms included end-of-life ethics, letting die, euthanasia, withholding treatment, withdrawing treatment, doctor–patient decision-making, and principles of biomedical ethics. The search identified 162 records. After removal of duplicates and screening of titles and abstracts for relevance to ethical analysis, 74 publications were retained for full-text review. Of these, 42 sources were selected for final analysis based on their explicit engagement with normative reasoning concerning end-of-life clinical decisions.
Inclusion criteria prioritized peer-reviewed journal articles, foundational bioethics texts, and professional ethical guidelines addressing the moral distinction between letting die and euthanasia. Studies focused primarily on technical medical outcomes or purely legal commentary without substantive ethical analysis were excluded. The selected literature was examined through qualitative content analysis, identifying recurrent ethical categories including intentionality, causation, autonomy, beneficence, non-maleficence, justice, and professional responsibility. A hermeneutic interpretive framework guided the analysis, situating ethical arguments within broader philosophical and clinical contexts and enabling critical engagement with underlying assumptions concerning human dignity, suffering, and moral agency.
However, as a normative literature review, the study does not generate empirical data and relies on the scope of published bioethical scholarship. Interpretive synthesis may involve scholarly judgment; however, this approach remains appropriate for clarifying conceptual distinctions and evaluating ethical reasoning in end-of-life decision-making.
4. Discussion
The literature consistently underscores that end-of-life ethical decision-making is multifaceted, context-dependent, and deeply relational. Letting die is generally accepted when aligned with patient autonomy and proportionality of care, whereas euthanasia remains ethically contested due to its intentionality. Ethical theories, such as
Doctrine of Double Effect duties, offer conceptual tools that support nuanced moral reasoning, helping doctors distinguish between permissible omissions and morally contentious acts. Moreover, professional codes operationalize these theories, providing concrete guidance that governs doctor–patient interactions and ensures accountability, moral integrity, and patient-centered care. Scholars emphasize that effective communication, shared decision-making, and ethical education are critical to navigating these complex ethical landscapes
| [21] | M. A. Alanazi et al., “Navigating end-of-life decision-making in nursing: a systematic review of ethical challenges and palliative care practices,” BMC Nurs., vol. 23, no. 1, 2024,
https://doi.org/10.1186/s12912-024-02087-5 |
| [22] | J. J. Thomson, “Killing, letting die, and the trolley problem.,” Monist, vol. 59, no. 2, 1976,
https://doi.org/10.5840/monist197659224 |
[21, 22]
. Collectively, the literature reveals that a principled, context-sensitive approach is essential for ethically defensible and clinically appropriate end-of-life care.
4.1. Integration with Ethical Theories and Professional Codes
The ethical frameworks discussed in the literature do more than provide parallel explanations of end-of-life decision-making; they reveal a deeper conceptual tension concerning how moral responsibility in medicine should be understood. Much of the ethical reasoning that distinguishes letting die from euthanasia ultimately rests on the role attributed to moral intention. The DDE remains central because it frames the ethical permissibility of clinical actions not by their outcomes alone but by the agent’s intention and the proportionality of the good pursued. Within this logic, actions such as administering high-dose analgesia or withdrawing disproportionate treatment are considered ethically permissible because death is neither the means nor the intended goal, but a foreseen consequence of relieving suffering. In clinical settings, this intention-based reasoning functions as a moral safeguard that allows physicians to respond compassionately to suffering without crossing into deliberate life termination.
Yet the literature also reveals the limits of relying exclusively on intention as the decisive moral criterion. Critics argue that in practice the boundary between foreseeing and intending death can become ethically ambiguous, particularly when actions predictably shorten life. Here, Ross’s theory of Prima Facie Duties provides an important corrective. Rather than grounding ethical judgment in a single principle, this framework recognizes that clinicians operate within a plurality of competing obligations—including beneficence, non-maleficence, fidelity, and respect for autonomy. Ethical deliberation therefore becomes a process of balancing morally relevant duties rather than applying rigid rules. In end-of-life contexts, this pluralistic approach better reflects the realities of clinical practice, where physicians must simultaneously alleviate suffering, respect patient wishes, and preserve the moral integrity of medicine.
Professional codes of ethics translate these philosophical insights into institutional standards. By affirming both the prohibition against intentional killing and the legitimacy of withdrawing disproportionate treatment, these codes institutionalize a normative boundary that preserves the physician’s identity as a healer while acknowledging the limits of medical intervention. The tension between relieving suffering and preserving life is therefore not eliminated but structured through ethical norms that guide professional judgment.
Taken together, these frameworks reveal that the ethical distinction between letting die and euthanasia does not depend on a single principle but emerges from the interaction of intention, professional responsibility, and relational obligations within clinical practice. The conceptual contribution of this study lies in clarifying this interaction: rather than viewing ethical theories as competing explanations, they can be understood as complementary layers of moral reasoning. The DDEclarifies the role of intention, prima facie duties illuminate the balancing of competing obligations, and professional codes institutionalize these insights within medical practice. This integrated perspective helps explain why letting die remains ethically defensible within medicine while euthanasia continues to challenge the moral boundaries of the profession.
4.2. Ethical Challenges in Doctor Decision-Making
The findings of this study indicate that the ethical distinction between letting die and euthanasia cannot be adequately understood through outcome-based reasoning alone. Although both practices may culminate in the patient’s death, the moral evaluation of these actions hinges on deeper questions concerning intention, moral agency, and the professional identity of medicine. Across the literature analyzed, the permissibility of letting die is consistently grounded in the convergence of three normative conditions: respect for patient autonomy, proportionality of medical intervention, and the physician’s duty to avoid intentional harm. When life-sustaining treatment is withdrawn because it is futile or disproportionately burdensome, death is attributed to the progression of the underlying illness rather than to the clinician’s agency. In this sense, letting die represents not an abandonment of care but a recognition of the limits of medicine.
Euthanasia, by contrast, introduces a fundamentally different moral structure. The act does not merely permit death but intentionally brings it about as the means of relieving suffering. This shift from allowing death to occur to causing death as an intervention relocates moral responsibility from the natural course of illness to the deliberate agency of the physician. It is precisely this relocation of agency that explains why euthanasia remains ethically contested even in contexts where compassion and patient autonomy are invoked as justificatory grounds. Critics argue that when the physician becomes the direct agent of death, the traditional ethical orientation of medicine—as a profession committed to healing, relieving suffering, and accompanying patients through illness—is profoundly reconfigured
.
The literature further reveals that ethical reasoning at the end of life is shaped by an unresolved tension between autonomy-centered ethics and professional role morality. Contemporary bioethics increasingly emphasizes patient self-determination, affirming the right of competent individuals to refuse treatment and to participate actively in decisions about their care. Empirical evidence demonstrates that structured communication and shared decision-making significantly enhance the alignment between medical care and patient preferences while reducing decisional conflict and psychological distress among patients and families
| [48] | M. J. Silveira, S. Y. H. Kim, and K. M. Langa, “Advance Directives and Outcomes of Surrogate Decision Making before Death,” New England Journal of Medicine, vol. 362, no. 13, 2010, https://doi.org/10.1056/nejmsa0907901 |
[48]
. However, when autonomy is interpreted as extending to a demand for life-ending intervention, it begins to collide with the physician’s duty of non-maleficence and with the professional norms that historically define the practice of medicine. The ethical challenge therefore lies not in choosing between autonomy and professional integrity, but in determining how these commitments can be reconciled without collapsing the moral boundaries that structure medical responsibility.
A further tension emerges between compassion and moral limits in clinical care. Both the withdrawal of futile treatment and the request for euthanasia are frequently motivated by a desire to alleviate suffering. Yet the ethical frameworks examined in this study—particularly the DDE and Prima Facie Duties—suggest that compassion alone cannot determine the moral permissibility of clinical actions. Instead, ethical justification depends on whether the relief of suffering is pursued through actions consistent with the moral vocation of medicine. In the case of letting die, the physician remains committed to care through palliative support, symptom relief, and accompaniment. In euthanasia, however, suffering is addressed through the direct termination of life, thereby altering the ethical meaning of the physician’s role.
The conceptual contribution of this study lies in clarifying that the distinction between letting die and euthanasia is best understood as a boundary of moral agency within medical practice. Rather than treating the distinction as merely procedural, legal, or outcome-based, the analysis demonstrates that it reflects a deeper normative structure that integrates intention, professional responsibility, and relational ethics. Letting die preserves the physician’s role as a moral agent who recognizes the limits of intervention while remaining committed to alleviating suffering. Euthanasia, by contrast, transfers the locus of death from the course of illness to the deliberate action of the clinician, thereby redefining the moral authority and identity of the medical profession.
Recognizing this distinction has important implications for clinical practice. Ethical clarity in end-of-life decision-making depends not only on abstract principles but also on institutional support structures that enable reflective moral deliberation. Ethics consultation services, communication training, and structured advance care planning can strengthen the capacity of clinicians to navigate these dilemmas while maintaining trust within the doctor–patient relationship. Ultimately, ethically defensible end-of-life care requires a framework that integrates respect for patient autonomy with the preservation of the moral commitments that define medicine as a profession of care rather than life termination.
4.3. Doctor–Patient Relationship and Shared Decision-Making
The findings and extant literature converge on a critical insight: the ethical soundness of end-of-life care is inextricably linked to the quality of communication and the practice of shared decision-making. Empirical studies consistently demonstrate that structured clinician–patient dialogue does more than convey information—it transforms ethically fraught decisions into deliberative processes that balance clinical expertise with patient values. For example, Rietjens
reports that shared decision-making interventions can increase patient knowledge by 19–25% and reduce decisional conflict by up to 30%, underscoring the tangible impact of communication on ethical clarity. Yet, this evidence also highlights an underlying tension: while clinicians often assume that informed consent is being met through the provision of information alone, many patients remain inadequately prepared to make complex choices, creating a gap between procedural consent and genuine ethical engagement.
This gap is further evidenced by studies showing that 40–60% of patients fail to fully understand their prognosis without structured communication interventions
. Such deficits not only compromise patient autonomy but also threaten the moral defensibility of clinical decisions, revealing a persistent ethical tension in standard care practices. In response, advance care planning emerges as a pivotal mechanism to mediate this tension: documented advance directives are associated with a 25–35% reduction in unwanted life-sustaining treatments and a 20% increase in alignment between patient preferences and actual care
| [48] | M. J. Silveira, S. Y. H. Kim, and K. M. Langa, “Advance Directives and Outcomes of Surrogate Decision Making before Death,” New England Journal of Medicine, vol. 362, no. 13, 2010, https://doi.org/10.1056/nejmsa0907901 |
[48]
. These data suggest that anticipatory dialogue functions as both a preventive and corrective strategy—anticipating ethical dilemmas while ensuring that patient values meaningfully shape clinical actions.
From the clinician’s perspective, shared decision-making provides a structured framework to navigate the dual obligations of respecting patient autonomy and exercising professional judgment. Surveys indicate that clinicians who regularly employ these strategies report a 15–20% increase in confidence regarding ethical clarity in end-of-life care
. This highlights a conceptual insight: communication is not merely a procedural or technical skill but a moral practice that operationalizes trust, accountability, and ethical alignment in care relationships.
Conceptually, this body of evidence illuminates a critical contribution to the ethics of clinical practice: the integration of structured communication and advance care planning constitutes a dual lever that simultaneously strengthens patient autonomy and mitigates moral tension in the clinical encounter. By positioning communication as both an empirical and normative axis, this framework reconceptualizes end-of-life care as an ethically co-constructed process—where deliberation, comprehension, and value alignment collectively constitute the foundation of morally defensible decision-making. In essence, the literature underscores that ethically sound end-of-life care is less about unilateral clinical expertise and more about orchestrating a transparent, reciprocal, and value-informed dialogue that resolves the inherent tensions of care at life’s threshold.
5. Communication and Advance Care Planning Framework at End-of-Life
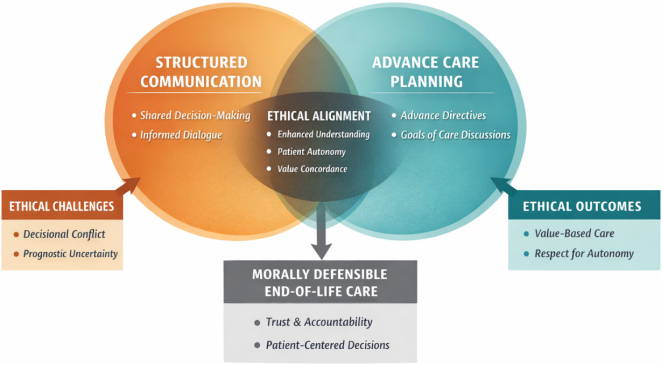
The conceptual framework situates ethically sound end-of-life care at the intersection of structured clinician–patient communication and advance care planning. Central to this model is the notion that ethical clarity and moral defensibility are not inherent properties of clinical interventions, but rather emerge from deliberate, value-informed processes that align patient preferences with clinical action. Structured communication—including shared decision-making and informed dialogue—facilitates patient comprehension, reduces decisional conflict, and operationalizes autonomy as an actionable principle within clinical encounters. Advance care planning, through documented directives and anticipatory goals-of-care discussions, ensures that patient values are both anticipated and respected, thereby bridging the temporal gap between preference articulation and clinical implementation. The intersection of these two domains—termed Ethical Alignment represents the conceptual contribution of the framework. Here, enhanced understanding, value concordance, and patient autonomy converge to mediate the moral tensions inherent in end-of-life decision-making. The framework highlights those ethical outcomes, such as respect for autonomy and the delivery of value-based care, are contingent upon the integration of these mechanisms rather than isolated interventions. Simultaneously, it acknowledges the persistent challenges of decisional conflict and prognostic uncertainty, illustrating the dynamic tension between ethical ideals and practical constraints in clinical contexts.
By positioning communication and planning as dual levers, the framework provides a pragmatic roadmap for morally defensible practice. It emphasizes that the ethical quality of end-of-life care is both an empirical and normative construct: structured dialogue and anticipatory planning empirically enhance patient comprehension and concordance, while normatively reinforcing trust, accountability, and shared moral responsibility in the clinician–patient relationship. Consequently, this integrative model offers a theoretically robust and actionable foundation for aligning clinical interventions with patient values, mitigating moral conflict, and advancing the ethical rigor of end-of-life care.
As illustrated in
Figure 1 structured clinician–patient communication and advance care planning function as dual mechanisms that enhance patient comprehension, align clinical actions with patient values, and mitigate moral tension. Ethical alignment emerges at the intersection of these processes, operationalizing autonomy, trust, and shared decision-making as central components of morally defensible end-of-life care.
Figure 1. Resolving Ethical Tension at the End of Life.
6. Conclusion
End-of-life decision-making remains among the most demanding responsibilities in clinical practice, requiring careful moral discernment rather than categorical judgments. This review reinforces that the ethical distinction between letting die and euthanasia is substantive. Withholding or withdrawing disproportionate or futile treatment can be morally justified when grounded in patient autonomy, proportionality of care, and fidelity to professional integrity, whereas euthanasia continues to provoke ethical controversy due to its intentional termination of life and the profound questions it raises about the moral identity and limits of medicine.
The original contribution of this study lies in contextualizing these ethical principles within the African healthcare environment, where resource constraints, cultural values, and systemic inequities uniquely shape end-of-life decision-making. It highlights the necessity of structured reasoning—anchored in autonomy, beneficence, non-maleficence, justice, and the DDE while emphasizing relational aspects such as transparent communication, shared decision-making, and advance care planning. These are not merely procedural tools but moral practices that safeguard dignity, reduce decisional conflict, and strengthen trust, particularly in settings where familial and community expectations intersect with professional obligations.
To advance ethical clarity in African healthcare systems, institutions must prioritize comprehensive ethics education, accessible consultation services, and communication training as integral clinical competencies. Moreover, research must explore underrepresented contexts, including longitudinal studies on how end-of-life decisions affect clinicians’ moral reasoning and professional identity. By foregrounding principled reasoning and relational attentiveness within culturally and resource-sensitive frameworks, this study contributes a nuanced ethical lens for end-of-life care that is both globally informed and locally grounded, reinforcing respect for human dignity at the point of life’s most vulnerable moments.